|
|
HYPERBARIC
OXYGENTHERAPY |
|

To
my friend Paulo Eduardo Iazzetti, MD, PhD, in Memorian.
Then unit chief from Hyperbaric
Service - Clinical
Hospital
State University of Campinas (SP)
- Brazil
*The origin of the hyperbaric medicine becomes related with the exploration of the subaqueous environment. Had occurred gradual attempts to surpass the limitations of the aquatic way, with the equipment use that allowed to increase the time of immersion or reached depth. The individual equipment use of diving, already was designated for the fenícios in century IX a.C.. The diving bells had been told by Aristotle in 325 a.C.. In 1662 Henshaw described the immersion bell, with ventilation system the bellows (Figures 1 and 2). Click
in the figures to extend it. Information on diving suits, with air provision coming of the surface, authorizing submersion of bigger permanence, date of century XVII. In century XIX, with efficient the individual equipment development of diving (Figure 3) and use of pneumatic tubuloes in workmanships of construction of bridges and mines, the potential and limitations in the exposition of the man to the subaqueous or pressurized environment had been delineated. Click
in the figures to extend it. Had the pathologie related with subaqueous or pressurized environment, the intervention of doctors and researchers became necessary. It is historical landmark, the work of the French fisiologista Paul Bert, that in 1876 published the workmanship "the Barometric Pressure", origin of the hyperbaric physiology and base of the modern hyperbaric medicine. The work of Paul Bert created the dedicated medical area to the study of the physiological and metabolic alterations of the displayed organism the superior pressures to the atmospheric pressure and systemize the hyperbaric oxigenoterapia, using the inhalation of pure oxygen in pressurized environment. The dutch surgeon Ite Boerema, in the decade of 1960, published article on the systematic use of the hyperbaric oxigenoterapia in the hospital way. The
Professor Alvaro
Ozório de Click in the figures to extend it.
Figure 4 The hyperbaric medicine is subdivided in two areas. One of them is dedicated to the professional activity and occupational health of divers (saturation diving), aeronauts and workers under air-tablet, therefore on to the medicine of the work. To another area of the hyperbaric medicine it is come back to the clinical application of the hyperbaric oxigenoterapia in hospital environment. Its challenge is the research and systematization of protocols that demonstrate, with scientific severity, the clinical potential of this therapeutical one.
In the procedure of the HBO the customer must be in the interior of the pressurized hyperbaric chamber. The HBO chambers can be monopatient or multipatients (Figures 6, 7). Click in the figures to extend it.
Figure 6
Figure 7 The hyperbaric chamber multipatients (Figure 7) holds, of simultaneous form, some people, also the doctor and/or specialized nurse. The mechanism of pressurization and despressurization is carried through with compressed air and the oxygen the 100% is inspired by means of mask or special pointed hood. The chambers monopatient (Figure 6) allow the room of only one customer, are pressurized by the pure oxygen, not having necessity of special devices for the inspiration of the O2. It has daily pay-established limits of exposition to the HBO, referring to the level of pressure and period of permanence in the interior of the chamber, therefore collateral effect will be able to occur undesirable, involving determined e regions agencies of the body. Before initiating the hyperbaric oxigenoterapia, the customer will have to be submitted to anamnese and complete clinical examination, with particular attention to the pulmões and timpanic membrane. The patient will have to be informed on all the measures of security, such as: use of adequate clothes (antifire) and to spoil itself of any personal effect that can originate fagulha electric, therefore the oxygen is highly inflammable. |
*The atmosphere consists of a gaseous mixture, contends in volume 20.94% of oxygen, 78.08% of nitrogen, about 0,04% of carbon dioxide and traces of gases, as argon, helium and krypton. Air that we breathe, therefore, in practical terms, is composed for 21% of oxygen and 79% of nitrogen. Click in the figures to extend it. The Dalton's Law determines that the partial pressure of a gas, component of one mixes, either proportional its fraction in this mixture (Figure 8). Of this form, an aerobic organism is submitted to a partial pressure of oxygen determined for the altitude where if it finds. Being the total pressure of the mixture in the level of the sea of 760mmHg, the partial pressure of the oxygen will be of 160mmHg. Figure 9 The gases are become fluid in the liquids of directly proportional form to the pressure, in accordance with the Henry's Law, and each gas presents one definitive coefficient of solubility in a specific liquid. The classic analogy to explain such phenomenon what it happens with the champagne bottle, when is opened. The pressure inside of it, that it was great, diminishes to the contact with the atmosphere and the gas, physically dissolved, is gotten loose (Figure 9). The coefficients of gases solubility, in the important corporal water and liquids, are variabily. Therefore, in the body temperature the solubility coefficient of the oxygen is 0,024ml/L/mmHg, the carbon dioxide is 0,57ml/L/mmHg and the nitrogen is 0,012ml/L/mmHg, being, therefore, the carbon dioxide twenty times more soluble than the oxygen. Of this form, after the dissolution of 0,024ml of oxygen in one liter of water, in constant temperature, will not be more possible to add gas to the solvent, in the atmospheric pressure. In normal physiological conditions the hemoglobina, that transport 200ml of oxygen in one liter of blood, regulates the necessity of the demand of this gas, being able the organism if to adapt the lesser partial pressures of oxygen, such as the existing one in great altitude, simply increasing the production of circulating hemacias. Figure 10
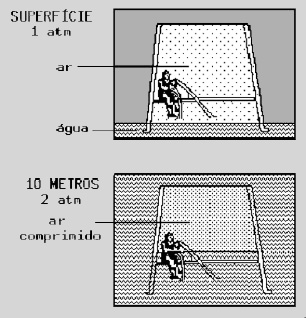
The Boyle's Law establishes that the pressure is inversely proportional to the volume of the gas (Figure 10). In the cylinder A we have It one liter of air in absolute atmospheric pressure (1ATA). in cylinder B, in case that embolo (piston) has an area of 1cm2, exerting a force of 1kgf, the pressure will be of 1kg/cm2, that it is equivalent the 1 atmosphere approximately; as already it had 1ATA in the environment, the resultant absolute pressure is of 2ATA. In this in case that, the volume scrumbles it the half. In cylinder C the pressure is of 3ATA and the volume is reduced to 1/3. In cylinder D the volume is of one room, since the pressure is of 4ATA.
*The hyperbaric oxygentherapy (HBO) consists of the oxygen inhalation at 100%, with superior pressure to the atmospheric pressure in the level of the sea. The hyperbaric medicine, generally, works with the cited ambient pressure in absolute atmospheres (atm abs or ATA). In the level of sea 1 atm abs is equivalent 760mmHg (1 ATA = 760 mmHg). The HBO demands that the patient remains in the interior of stamped compartments, resistant to the hyperbaric pressure, chambers. It has immediate therapeutical value only in cases of gaseous embolism or disbarics pathologie, as the descompressive illness. The treatment of the HBO has for primordial factor the increase of the tension of oxygen in the corporal liquids. If the patient, submitted to the treatment of HBO, inhaling oxygen 100 %, for example, to the 3ATA pressure will be able to reach until the value of 2.000mmHg. In this hypothesis, about 6,4ml of oxygen will be dissolved in each 100ml of blood, beyond the on O2 already to the hemoglobina. The HBO provokes available free substratum increase, or either, increase of the production of activated radicals. Some tissue are more susceptible the oxidative injuries, being able to provoke not wished disfunction. Beyond the pulmonary toxic action of the O2, whose chronic or subacute effect well are known, the central nervous system can present important and acute alterations. Paul Bert, in 1878, described the acute neurotoxic action of the O2, that presents the phases prodromic and convulsive. In the first phase (prodrômica) attended the manifest discomfort and symptoms neuropsicomotores, already, in the convulsive phase appear contractions tonic-clônicas and loss of conscience, resembling themselves it the classic epilética crisis. The neurotóxica crisis of the O2 can happen in patients who have been submitted to the OHB, with the equal or superior pressurization 3ATA. More recent studies had indicated the envolvement of nitric oxide as mediating in the neurological toxicidade of the hyperbaric oxygen. The HBO can provoke pulmonary alteration, in reason of the high tensions of oxygen which the lung is submitted, therefore how much bigger the pressure of this gas in the lung, greater amount of O2 will be absorbed by the blood and dissolved in the corporeal liquids. Ahead of these secondary effect of the hyperbaric oxygentherapy, it has daily pay-established limits of exposition to this therapy, referring to the level of pressure and period of permanence in the interior of the chamber.
*The mechanical effect of the increase of absolute the atmospheric pressure during the procedure of the HBO can correspond the barotraumas of the sockets filled for air, such as lung, heard average and seios of the face. 1.
Barotrauma middle ear: He is composed for some structures, each one with specific function: the timpanic membrane (Figure 11-a) receives the stimulatons auditory from the external way, that will be transmitted to the spandrel. The middle ear is communicated with nasofaringe, by means of the membranoso canal, also called tube of Eustaquio (Figure 11-b)
Figure 11 Barotrauma of the middle ear is subject to the variations of barometric pressure of the environment, being able to also provoke the rupture of the timpanic membrane (Figure 11-a). To prevent this problem, the patient to be submitted to the treatment of hyperbaric oxygentherapy is guided to carry through the "Valsalva Manoeuvre", that she promotes equalization of the pressure difference enters the external way (hyperbaric chamber) and the internal ear. The maneuver, described for the Italian physiologist Valsalva, consists of the act of the patient to provoke the expiration mechanism, keeping the closed mouth and covered nose as the fingers, thus, the air, that would have to be exhaled, passes through the tube of Eustaquio (Figure 11-b) for the internal ear. 2.
Sinusal Barotrauma: The main sinusals sinus are: frontal (Figures 12-1 and 13-a), esfenoidal (Figure 12-2), to maxilar (Figure 13-b) and paranasal (Figure 13-c). Click in the figures to extend it.
Figure 12 Figure 13
The sinus of the face are communicated by means of membranosos canals with nasofaringe. They are citizens to the variation of barometric pressure during the HBO procedure. When the membranosos canals are obstructed by secretion, the physiological equalization between the chamber pressures and external it could be made it difficult, being able to cause local pain and hemorrhage. 3.
Pulmonary Barotrauma:
Figure 14 Some of these tissue are sensible to the variation of atmospheric pressure during the HBO procedure, being able to occur bleed and enfisema during extreme the hyperbaric exposition. 4.
Traumatic Embolism Caused by Air: In case that the attended one inspires the hyperbaric oxygen and holds back the breath in apnea and, accidentally, fast despressurization of the hyperbaric chamber, the lung occurs, for the reduction of the external pressure, will be submitted to the sudden expansion, that provokes increase of its pulmonary chamber pressure and alveolar rupture (pulmonary barotrauma). In
this hypothesis, the rupture of the pulmonary alveoli can provoke: This accident is called traumatic embolism provoked by air. More it is related to the activity of diving of that to the clinical hyperbaric medicine. |
*The therapeutical potential potential of the hyperbaric oxygenation elapses of the absorption of high dose of oxygen, that can compensate definitive conditions of hipoxia, modifying the evolution of the illness. Some
mechanisms are of particular interest for the medicine, such as:
*Bibliographical
Reference:
The hyperbaric hiperoxia have peculiar vasoconstritor effect in the majority of tissue. This effect must to the intrinsic vasomotor control, with little influence of the mechanisms central offices. Generalized vasoconstriction occurs, being exception the pulmonary circulation, a time that the hyperbaric hiperoxia provokes pulmonary vasodilatation The vasoconstriction takes advantage in greater or minor in agreement degree the type of fabric, provoking increase of the peripheral vascular resistance and dislocating the sanguine volemia for the capacitance vases, diminishing, thus, the venoso return. The hiperoxia induces to the reduction of the cardiac frequency. The combination of these effect reduces the cardiac debit, in approximately 20 30% with pressurization of 3ATA. Although the peripheral vascular resistance increases with the procedure of the hyperbaric oxygentherapy, the arterial pressure is kept, due to proportional reduction of the cardiac debit.
The alterations of the central nervous system in hyperbaric hiperóxia initially correspond to the period of activation, that occurs enters the 60 to 90 minutes in the pressure of 2 to 3ATA. Cognitivos and percipient tests, carried through in patients submitted to the HBO, had demonstrated to performance after the treatment better. Active the hyperbaric hiperóxia the reticular formation of ascending and descending the central nervous system, with manifestations. The descending manifestation if relates the biggest excitabilidade to medular, provoking increase of tônus muscular. The ascending activation of the reticular formation provokes endicrine alterations, through the hipotalamo-hipofisary axle, with adeno-cortico-trofico hormone release (ACTH), leading to the increase of adrenais corticoids e, by means of the direct stimulation of the adrenal cortex, also of the epinefrina. Normally, the application of the HBO, with therapeutical severity, demands clinical attention on these alterations only in susceptible patients. In the patient citizens the expositions in the maximum limits of HBO the neuro-endócrinos effect will be exacerbados, supervening neurotoxic symptoms.
The global consumption of oxygen in hyperbaric hiperóxia is remained unchanged. This happens because, during the 30 to 60 initial minutes of exposition, the oxygen if spreads out for all corporal tissue, until saturating them, substituting nitrogen, in impregnated them, that it is eliminated by diffusion. If they will be effected measured of consumption of oxygen in this phase, the O2 pparently will be increased. In the state of hyperbaric hiperóxia the present hemoglobina in the venoso blood can be partial or total saturated of O2. About 20% of the carbon dioxide (CO2), that they would be carried by the hemoglobina, will be dissolved in the plasma, forming bigger acid amount of carbonic, having, therefore, addition to be tamponado by the bicarbonate system. Existing sufficiency of this mechanism, significant alterations of pH or pCO2 (partial pressure CO2) will not occur sanguine. In the metabolism pro-oxidante and antirust reactions occur, still, that must be kept in balance, hindering that the excess of oxidation or comprometimento it system of antirust protection can lesionar complete cells. The set of these mechanisms is called oxidativo metabolism. The biggest concentration of oxygen, proportionate for the hyperbaric hiperoxia, increases the formation of radicals activated of O2, stimulating the oxidative reactions and antirust systems. These same manifestations can occur in the exposition drawn out to the oxygen the 100% in normobaric pressure, however, of faster and sharp form in the HBO. It has, however, peculiar toxic effect of the hyperbaric oxygentherapy, as neurological alterations, that do not occur in normobaric hiperoxia. The alterations of the oxidative rocking produced by the hyperbaric hiperoxia, can be evaluated by the dosage of pulmonary antirust enzymes.
Diverse pathological conditions can diminish the tension of oxygen in the affected place. The bacterial development is favored by the hipoxia or anaerobiosis. The hyperbaric hiperoxia favors the action bacteriostática, modifying, for example, amino acid biosynthesis, diffusion of the membrane and synthesis and degradation of DNA of the bacteria. Bacterial sensitivity in relation to the oxygen tension is changeable, being more evident in the anaerobics bacteria.
It
Consults
the Feridologo's
|
*Countless they are the indications of HBO determined by several protocols accepted internationally: 1. Gas clots, 2. Decompression sickness, 3. Traumatic air clot, 4 .Carbon monoxide or smoke intoxication, 5. Cyanide or cyanide derivatives poisoning, 6. Clostridial gas gangrene, 7. Fournier syndrome, 8. Necrotic Fasciities and other necrotic infections, 9. Traumatic acute ischaemias: crush lesion, compartmental syndrome, reimplantation of amputated extremities, 10. Limbs or grafts that are damaged or at risk, 11. Acute vasculites of allergic, medicinal aetiology or caused by biological toxins (arachnids, ophidians and insects), 12. Complex burn, 13. Refractory lesions: pressure ulcers, vasculogenic, neuropathic (diabetic foot), etc, 14. Lesions from radiation: radiodermitis, osteo-radionecrosis and actininc lesions, 15. Chronic osteomyelitis, 16. Hypoacusia from ototoxicity to chemiotherapy agents, 17.
Sharp anemia in the cases of impossibility of sanguine
transfusion,
Click in the
photo to see the
1. Candido LC, Iazzetti PE.: Tratamento Das Feridas Cirúrgicas Pós-Fasciites Necrotizantes. Rev.Esc.Enf.USP, 33(Esp):229-230, 1999. 2. Candido L.C., Pellissari M.B.P., Leite M.S., Vinhaes E.G., Iazzetti P.E.: Tratamento das Feridas Pós-Síndrome De Fournier”. Rev.Esc.Enf.USP, 33(Esp):211-213, 1999. 3. Candido L.C., Aplicação da Oxigenoterapia Hiperbárica na Fasciite Necrotizante dos membros - Abordagem Interdisciplinar no Tratamento de Feridas. In abstract-books, IX Congresso Italiano de Microcirurgia Reconstrutiva, pág. 21, 2000. 4. Candido L.C.: “Aplicação da Oxigenoterapia Hiperbárica no Tratamento de Feridas”. IV Congresso Brasileiro de Estomaterapia e I Congresso Brasileiro de Enfermagem em Dermatologia, São Paulo (SP), 2001. 5. Candido L.C.: Topical Treatment of Wounds From Poisonous Animals’ Bites and Stings. 14° Biennal Congress World Council of Enterostomal Therapists (WCET), Florence – Italy, 2002. 6. Candido L.C.: “Upper Limb Reconstruction after Complex Burns. Alternatives in Topical Therapy. 14° Biennal Congress World Council of Enterostomal Therapists (WCET), Florence – Italy, 2002. 7. Candido L.C.: Topical and Surgical Treatment of Lesions Post-Necrotic Fasciities. 14° Biennal Congress World Council of Enterostomal Therapists (WCET), Florence – Italy, 2002. 8. Candido L.C.: Treatment of Refractory Vasculogenic Lesions. 14° Biennal Congress World Council of Enterostomal Therapists (WCET), Florence – Italy, 2002. 9. Candido L.C.: Topical and Surgical Treatment of Post-Fournier Syndrome Wounds. 14° Biennal Congress World Council of Enterostomal Therapists (WCET), Florence – Italy, 2002. 10. Candido L.C.: The Application of Hyperbaric Oxygen Therapy in the Treatment of Wounds. 14° Biennal Congress World Council of Enterostomal Therapists (WCET), Florence – Italy, em 10.07.2002. 11. Candido
L.C.: Topical
and Surgical Treatment of Neurogenic Diabetic Foot Ulcers.14° Biennal Congress
World Council of Enterostomal Therapists (WCET), Florence – Italy, 12. Candido
L.C.: Topical and Surgical Treatment of Vegetant Cutaneous Neoplasm. 14°
Biennal Congress World Council of Enterostomal Therapists (WCET), Florence –
Italy, 13. Candido L.C.: Topical and Surgical Treatment of the Pressure Ulcers. 14° Biennal Congress World Council of Enterostomal Therapists (WCET), Florence – Italy, em 10.07.2002. 14. Candido
L.C.: Topical and Surgical Treatment of Complex Traumatic Lesion with
Loss of Cutaneous Substance. 14° Biennal Congress World Council of Enterostomal
Therapists (WCET), Florence – Italy, 15. Candido L.C.: Lesões Traumáticas Complexas - Tratamento Tópico e Cirúrgico. In: Abstract Book do I Congresso da Sociedade Brasileira de Medicina Hiperbárica. Rio de Janeiro, pag. 7, 2002. 16. Candido L.C.: Síndrome de Fournier - Tratamento Tópico e Cirúrgico. In: Abstract Book do I Congresso da Sociedade Brasileira de Medicina Hiperbárica. Rio de Janeiro, pag. 9, 2002. 17. Candido L.C.: Fasciites Necrotizantes - Tratamento Tópico e Cirúrgico. In: Abstract Book do I Congresso da Sociedade Brasileira de Medicina Hiperbárica. Rio de Janeiro, pag.11, 2002. 18. Candido L.C.: Ferida Cirúrgica Pós-Fasciotomia. Tratamento Tópico e Cirúrgico. In: Abstract Book do I Congresso da Sociedade Brasileira de Medicina Hiperbárica. Rio de Janeiro, pag. 12, 2002. 19. Candido L.C.: Tratamento de Feridas Cutâneas Pós-Deiscência de Sutura Cirúrgica. In: Abstract Book do I Congresso da Sociedade Brasileira de Medicina Hiperbárica. Rio de Janeiro, pag. 13, 2002. 20. Candido L.C.: Queimaduras Complexas - Tratamento Tópico e Cirúrgica. In: Abstract Book do I Congresso da Sociedade Brasileira de Medicina Hiperbárica. Rio de Janeiro, pag. 14, 2002. 21. Candido L.C.: Lesões Cutâneas Provocadas por Mordedura de Animais Peçonhentos - Tratamento Tópico e Cirúrgico. In: Abstract Book do I Congresso da Sociedade Brasileira de Medicina Hiperbárica. Rio de Janeiro, pag. 16, 2002. 22. Candido L.C.: Neoplasias Cutâneas Vegetantes - Tratamento Tópico e Cirúrgico. In: Abstract Book do I Congresso da Sociedade Brasileira de Medicina Hiperbárica. Rio de Janeiro, pag. 19, 2002. 23. Candido L.C.: Úlcera Neuropática - O “Pé Diabético”. Tratamento Tópico e Cirúrgico. In: Abstract Book do I Congresso da Sociedade Brasileira de Medicina Hiperbárica. Rio de Janeiro, pag. 20, 2002. 24. Candido L.C.: Lesões Vasculogênicas Refratárias - Tratamento Tópico e Cirúrgico. In: Abstract Book do I Congresso da Sociedade Brasileira de Medicina Hiperbárica. Rio de Janeiro, pag. 21, 2002. 25. Candido L.C.: Úlceras de Pressão Refratárias - Tratamento Tópico e Cirúrgico. In: Abstract Book do I Congresso da Sociedade Brasileira de Medicina Hiperbárica. Rio de Janeiro, pag. 22, 2002. 26. Iazzetti P.E. Oxigenoterapia Hiperbárica. In: Anais de Atualização Médica, Medical Master. 3:73-84. 27. Iazzetti P.E.: Hiperoxigenação hiperbárica. In: Equilíbrio Ácido-Básico, Terzi R.G.G. (ed), 6:180-204, 1997. |